Cranial cruciate disease
Case example
Cranial cruciate disease
An 8 year-old, male castrated Leonberger was presented for right pelvic limb lameness, questionable positive drawer/stifle joint laxity and normal radiographs of the right stifle.
MRI findings
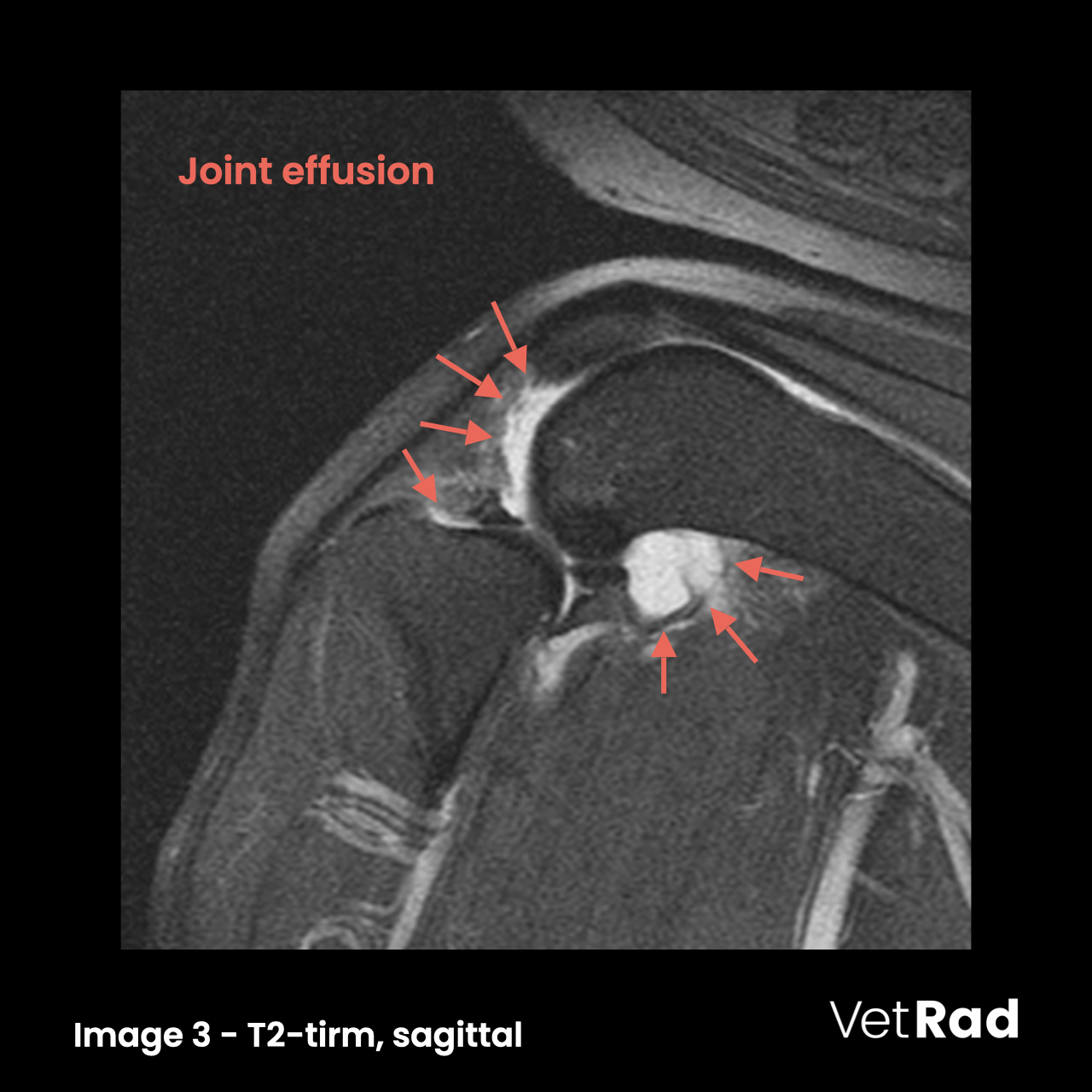
An amorphous, marked T2- and STIR hyperintense region is within the intercondylar fossa at the origin of the cranial and caudal cruciate ligaments. (Image 1) The cranial cruciate ligament (CrCL) is enlarged with irregular contours and T2- and STIR hyperintense signal. (Image 2) The joint is filled with homogenously intense fluid. (Image 3)


Conclusions
- Cranial cruciate desmitis with osseous oedema at its origin, the suspicion of a partial tear, mild, secondary stifle osteoarthrosis and joint effusion.
Learning points
- Magnetic resonance imaging (MRI) is the imaging modality of choice for evaluation of the cruciate ligaments, menisci and other stifle joint components due to its superior contrast resolution.
- Primary MRI findings in CrCL disease include abnormal signal intensity, fiber discontinuity or fiber distortion.
- Osseous oedema at the origin of the CrCL is a secondary sign and can be due to increased strain and secondary remodeling.
More information
- »Accuracy of 3 Tesla magnetic resonance imaging using detection of fiber loss and visual analog scale for diagnosing partial and complete cranial cruciate ligament ruptures in dogs«
— Fazio et al., Vet Radiol Ultrasound. 2018 Jan;59(1):64-78. - »Radiographic and magnetic resonance imaging predicts severity of cruciate ligament fiber damage and synovitis in dogs with cranial cruciate ligament rupture«
— Sample et al., PLoS ONE 12(6): e0178086.
Images courtesy of the AniCura Tierklinik Hollabrunn, Austria.
MEINE DATEIEN JETZT HOCHLADEN